| If you do
NOT see the Table of Contents frame to the left of this page, then
Click here to open 'USArmyGermany' frameset |
|||
|
Medical Division |
|||
|
|
|||
|
|||
|
|
|||
| USAREUR Medical Division | |||
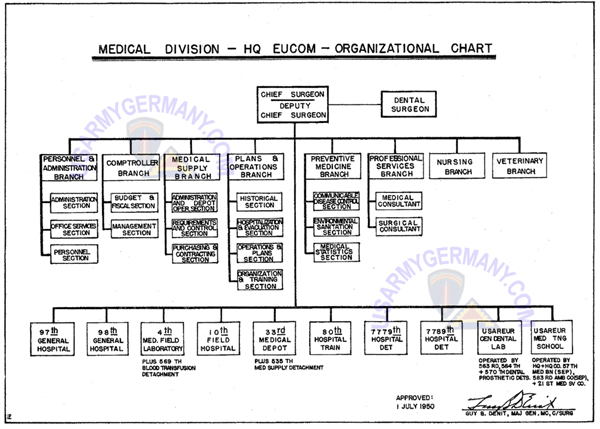 Organization of the Medical Division, European Command, 1950 |
|||
| 1950 | |||
| (Source: EUCOM Medical Bulletin, Sept 1950) | |||
| Organization and Functions of the Medical Division by Capt. Robert G. Valentine, MSG, and Lt. Fred W. Kelly, MSC The chart above reflects the current organization of Medical Division, Headquarters, EUCOM as of 1 July 1950. This article outlines the functions performed by the various branches and sections of the Medical Division. It is believed that familiarity with the organizational chart and the statement of functions may save time in avoiding misdirected inquiries, and should be of particular value to newly assigned officers who have not yet become fully familiar with the organization of the division. 1. CHIEF SURGEON 2, DEPUTY CHIEF SURGEON 3. DENTAL SURGEON 4, PERSONNEL AND ADMINISTRATION BRANCH Administration Section Office Services Section Personnel Section 5. COMPTROLLER BRANCH Budget and Fiscal Section Management Section 6. MEDICAL SUPPLY BRANCH Administration and Depot Operation Section Requirements and Control Section Purchasing and Contracting Section 7. PLANS AND OPERATIONS BRANCH Operations and Plans Section Organization and Training Section Hospitalization and Evacuation Section Historical Section 8. PREVENTIVE MEDICINE BRANCH Communicable Disease Control Section Environmental Sanitation Section Medical Statistics Section 9. PROFESSIONAL SERVICES BRANCH Medical Consultant Surgical Consultant 10, NURSING BRANCH 11. VETERINARY BRANCH |
|||
| 1957 | |||
| Source: USAREUR Medical Bulletin, May 1968) | |||
| Medical Service Areas Of particular interest is the reorganization of medical care in Germany under a new concept developed in the mid-50's. This is the Hospital Center-Medical Service Area organizational structure, an integrated system of health care implemented by the US Army Hospital Center, Germany, in 1957. The objective was more efficient utilization of medical resources. Using that most basic of managerial tenets - coequal responsibility and authority - the medical commander was given an overall job, to maintain the health of a geographical command, and control of the resources to do it. Central to the new organization was the satellization of the fixed dispensaries on existing field and station hospitals. Previously, the small medical units, staffed in most cases by young doctors with little or no military experience, too often had no experienced personnel to turn to for guidance. Under the new set-up, the small units were supervised by the experienced senior medical officers and their administrative staffs assigned to the major medical units (hospitals). |
|||
| 1970 | |||
| (Source: USAREUR Medical Bulletin, June 1970) | |||
| In USAREUR, there are about 115 dispensaries, 75 being on the USAREUR side and 40 on the Seventh Army side. | |||
| 1971 | |||
| (Source: USAREUR Medical Bulletin, January 1971) | |||
| The term dispensary has been a part of the Army as long as the Army Medical Corps has been in existence. But a change has taken place, and the term will no longer be used to define fixed ambulatory medical treatment facilities. Instead, the terms Troop Medical Clinic, Health Clinic, and Civilian Employees Health Clinic will be used. The
Department of the Army and The Surgeon General, in an attempt to better define the various duties of what were previously known as dispensaries, initiated the change on December 1.
The change, worldwide for all Army dispensaries, will effect only fixed ambulatory medical treatment facilities and activities. Those operated by individual units will continue to be known as dispensaries. The change will effect 78 individual clinics that fall under the United States Army Medical Command, Europe. The Troop Medical Clinic is defined as a medical treatment activity designed to accomplish sick call, and limited services including medical examinations, physical profiling and pharmacy dispensing. The former US Army Dispensary, Heidelberg, located at Patton Barracks, is now known as the US Army Medical Clinic, Heidelberg. The Health Clinic is a medical treatment activity equipped and staffed to provide ambulatory health services to eligible beneficiaries, to include active duty and retired military personnel and their dependents as well as dependents of deceased military personnel. Besides general radiology, laboratory, and pharmacy capabilities, it offers specialty medical care in one or more of the sub-specialties of medicine and dentistry. It may be equipped to handle a limited number of patients awaiting transfer to a hospital, and provide care (normally not to exceed 72 hours) for cases which cannot be handled on an outpatient status, but do not require hospitalization. The former US Army Dispensary, Mannheim, in Benjamin Franklin Village, is now called the US Army Health Clinic, Mannheim. The Civilian Employees Health Clinic promotes the health and fitness of civilian employees of the Federal Government. Its scope includes on-the-job illness or injury and dental conditions requiring emergency treatment. |
|||
| (Source: USAREUR Medical Bulletin, February 1971) | |||
| All USAMEDCOMEUR assigned hospitals are currently updating their TOE to the ''G" Series. | |||
| 1972 | |||
| (Source: STARS & STRIPES, March 21, 1972) | |||
| Medical Department Activities The U.S. Army Medical Comd-Europe's 14 medical service areas will be redesignated as medical department activities (MEDDAC) effective April 1. Except for general hospitals, U.S. Army hospitals in the United States and their affiliated health clinics, troop medical clinics, dental clinics and veterinary services have been under the MEDDAC concept since 1967. |
|||
| Fontainebleau Medical Depot | |||
 Main gate of Caserne Lariboisiere, Fontainebleau, 1960s (Earl Carter) |
|||
| 1953 | |||
| (Source: STARS & STRIPES, June 27, 1953) | |||
| The Fontainebleau Medical Depot is located at Caserne Lariboisiere in Fontainebleau, France. CO of the depot is Lt Col Roy E. Brooks. Since it opened in June 1950, the depot has served as the only reserve medical depot in Europe until the new medical depot at La Roche-sur-Yon in Western France was opened two months ago. (As a "reserve" depot, the operation was strictly a static receive and store activity with no further issuing of supplies to units.) The Fontainebleau depot has been part of the Communications Zone since December 1952, before that it was under the European Command headquarters. The depot is operated by the 33rd Medical Depot which will begin issuing medical supplies and equipment for Army and Air Force installations starting on July 1. With the opening in July, Com Z units will no longer depend upon the Rhine Medical Depot (Einsiedlerhof, Germany) for their supplies. With the new issue mission, the 33rd will supply 12 Army and Air Force accounts, which in turn will supply several satellite units. Included in the accounts are the general hospitals at Orleans (34th GH) and La Rochelle (28th GH). The 503rd Medical Det (one of the subordinate units of the depot) manufactures glasses for all Com Z personnel. With the new mission it will also provide optical supplies for Canadian air bases in France as well as US installations. The depot also operates a mobile refrigerator van which transports vaccines to stations throughout France. |
|||
| 4th Medical Laboratory (Field) | |||
| 1953 | |||
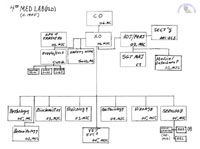
| (Source: Email from James E. Sullivan, 4th Med Lab, 1953-1956) | |||
I was stationed in Germany from late 1953 to 1956. I was with the Blood Bank of the 4th Med Lab (later the 10th?) at Landstuhl for 2-1/2 years and was on six months TDY as Lab Officer at the USAH in Bad Kreuznach.
My active service was for 7-1/2 years and I remained in the Active Reserve for the next 14 years, and my civilian occupation was in Hospital Administration.
I still remember many of the enlisted and officer personnel from that time and would be happy to recount a few of the events of that period. I'm attaching an Organization Chart to supplement the narrative; at least I can't get too long winded on it. I apologize for omissions of personnel and errors of the Org Chart.
|
|||
|
|||
|
The then designated 4th Medical Laboratory (Field) was commanded by COL Albert Richmond, who was succeeded by COL ___ Ernst who was in post when I rotated to CONUS in 1956. COL Richmond had retired and became Chief of Pathology at the Nix Hospital here in San Antonio and worked there for many years. He passed away ten or twelve years ago, though I may be in error here.
The mission of the 4th was to furnish Pathology Services to USAREUR Hospitals of all services that were beyond local capability. Blood Bank Services was for all service hospitals in the Western Area Command (WACOM), which was roughly between Pirmasens in the south, Baumholder in the north, and east to the Rhine River and west to the SAAR border. In the event of hostilities, the 4th was capable of simply packing up stored equipment and after augmentation of appropriate vehicles from the Post Motor Pool, displace to wherever assigned. There were small scale practice mobilization exercises during my tenure there and I have to say they were well organized and would tend to surprise the combat commanders that absorbed our technical people with our professionalism and motivation. Often we would hear comments such as "you mean you can really do Lab Tests and Blood Banking here in the field?" We were happy to give tours showing our capabilities were "good to go" as the saying is now. The monthly "alerts" in USAREUR were separate from the more comprehensive practice mobilization efforts of various units in the command. With respect to the 4th Med Lab, the only division that packed up fully were the Blood Bank Detachments. We had field type refrigerators that were trundled down some stairs to waiting trucks, and various chemicals and testing material were packed in insulated containers, and were driven up to the alert assembly area behind the main lab building. The other sections of the 4th were represented by trucks that would have been used in event of actual mobilization. It just wasn't feasible to pack up the whole chemistry or bacteriology or other component units and then unpack in an hour or two. The risk of losing or damaging specimens was too great for a morning exercise.
The Adjutant was CWO J.D. Hamil who was succeeded by CPT ____Thomas, MSC. The Enlisted Detachment Commander was CPT Harry Bolter. The 4th Med Executive Officer was a
COL _____ Kuhn
. He was also Chief of Bacteriology (now Microbiology); his assistant was 1LT Ken Borchardt. The Chief of Biochemistry was LTC Bob Krivulka, MSC;
1LT Wm. J. Campbell, MSC, Staff Biochemist.
1LT Evan Thomas, MSC, Bacteriology. The Chief of Serology (including Blood Bank) was LTC Frank W. Chorpenning, who retired to a professorship at Ohio State University. He was succeeded by LTC Charles Dunne, MSC. The staff officers at the Blood Bank were 1LT John W. Moose, MSC, 1LT George B. Edmonson, MSC, and yours truly. (Side Note: LT Moose married LTC Dunne's secretary, Frauline Hildegarde Gobel and they lived happily ever after.) The Blood Bank NCOIC was MSG____ Crenshaw. WO2 Frank Bremmerman was Blood Bank Admin. Officer and was the unofficial Blood Bank Supply Officer. SSG John Lancaster was Chief of the Bleeding Team techs, an a SSG ___Longo was the Blood Bank Lab NCOIC. The Blood Bank organization consisted of four then designated 8-500 TOE units, namely:
Shorthand for these units were BBB and BBL. The BBBs had 8-10 enlisted positions authorized plus the CO. If I recall correctly, in the event of mobilization for field duty, the Chief of Serology would remain on the Commander's staff for guidance in his area. The mobilized BBB and BBL units would be controlled operationally by the senior Medical Officer of the field units to which they would be attached. A LTC____ Fodor was Chief of Virology, and his assistant was LTC Conan Millstein. The next ranking MC Officer was Chief Pathologist MAJ William Williams from Annapolis, Md. He had a MAJ____ Pontius as his assistant, and a German Pathologist named Dr. Fett as second assistant. The Chief of Parasitology was 1LT Norman E. Wilkes who also doubled as Chief of Training. The Chief of Toxicology was LTC Glen Madera, MSC. I have forgotten the name of the Warrant Officer who was Chief of the 4th Med Supply and Services.
Chief of Veterinary Services was Major E. Wayne Grogan, VC. CAPT Robert Angel, MSC, Staff Biochemist. Capt. _____Walsh, MSC, Safety Officer. C APT______ Detwiler, MSC, Ass't. Safety Officer. I almost forgot to remember one of the more interesting Section Chiefs at the 4th, one LTC F.W. Whittemore, MSC who was Chief of Entomology. Besides being a premier "bug man" he was an expert planner in the area of disasters, mass casualties and he had a gift of making these subjects genuinely interesting. At some time in 1955 or early 1956 (memory serving) the unit was redesignated as the 10th Medical Laboratory (General) but nothing changed as far as the day to day operations went. I think the command responsibility was changed in that they were forming Medical Centers or some such and the Lab CO would report to the Center Commander instead of directly to what was called Medical Division, USAREUR. The posts'
name was changed from Landstuhl Army Medical Center (LAMC) to The 9th Hospital
Center, I think. The Center Commander when I arrived was a COL McConkie, and he was succeeded by COL Paul Hayes whose wife, LTC Katherine was Chief Nurse. Col Hayes was succeeded by COL____St. John shortly after I left and got a star soon after. The Post Executive Officer was a COL____ Hastings, who was the first full colonel in the MSC I ever knew. .
Of passing interest might be the fact that the first use of plastic bags for blood collection began by the Blood Bank in mid 1956 I believe. Up to then, the glass vacuum bottles were used but a big disadvantage was that they had to be transported to and from the unit donating blood in heavy ice chests and the rocking and swaying motion of the vehicles they were carried in tended to damage the red blood cells during the return journey, resulting in a shelf life of only 21 days per unit at that time. Plastic bags were soft and did not jostle around and cell damage was almost nil. The downside was that collection time was longer since blood was not "pulled" out of the veins with a vacuum bottle, but had to flow into the bag by gravity only. It took some getting used to but was a total success and is still the standard collection vessel to date.
Let me digress somewhat from the narrative to mention something that may add a little to these recollections. Before Gulf War II I had been in contact with the Public Affairs Officer of the Medical Center, a civilian lady. She had put a notice in the then Retired Officer Magazine that there was going to be a celebration of the Center's 50th anniversary and she asked for input from people who had been stationed there through the years. I sent her a couple of e-mails that astounded her as the information went beyond my particular unit, and she and I had quite an exchange of e-mails about the planned doings, and my wife and I actually planned on attending since we were planning a Space-A trip to Germany around that time. Then came the war, and that was the end of that. I'm thinking that the PAO at the Hq still may have archived our correspondence and perhaps you can check. I lost my copies when I got a new computer three years ago and the nerd I hired to save my files lost all my e-mail storage. A pity. |
|||
| 10th Medical Laboratory | |||
| 1958 | |||
| (Source: Email from James W. Legg, 10th Med Lab, 1958-1960) | |||
I was stationed w/ the 10th Med. Lab. from Dec. 1958 to Oct. 1960. I worked in the Chemistry - subsection Toxicology. At that time the Lab. CO was Col. Steer and when I arrived Capt. Trahan was OIC for Chem. and Tox was under Lt. Smith. Later Lt. Smith DEROSed & Lt. Crook replaced him.
When I arrived, the 4th Med. Lab. (Field) was a 7th Army Unit and the 10th was a COMZ unit. It was my understanding that the 10th was a forward unit from France. Later we both became USAREUR Med Lab. & wore the USAREUR patch. When I was there our tox. case load ran about 365/yr. I was back about 20 yr. later and they were doing about 1200/yr. Maj. Camp was over the Blood Bank. I ran into a Capt. Arnoldon - who was an enlisted man at the time and worked in Vet. Section Chem. - in Seoul. He had become a Blood Bank officer and had served w/ Col. (or LTC) Camp at Ft. Knox.
I had seen an article about a dentist puting a false tooth in a guard dog. This was in one of the free newspapers you get in Germany. The dentist was LTC Hans Berg who had worked as an EM in the chem. sect. with me.
On my transport on the USS Randall was SSG Philip Belmont. He was also assigned to the med. lab. in Micro. I had previously known him at Ft. Sam Houston as a Maj. He had been RIF'ed due age to retirement. At that time RIF'ed officers could opt to remain as an NCO until they completed their 20 yr.
I have been in contact with a few of the other EM that I served with in the past few years. |
|||
|
|
|||
| Related Links: CHAPTER XI: Redeployment and Occupation - Official historical manuscript that describes in some detail the U.S. Army medical supply system as it existed during World War II. Chapter XI covers the early Occupation period in Europe. |
|||